

Brain Bucket: a Social History of War, Football, Helmets, and Head Injury
A series for the playoff season
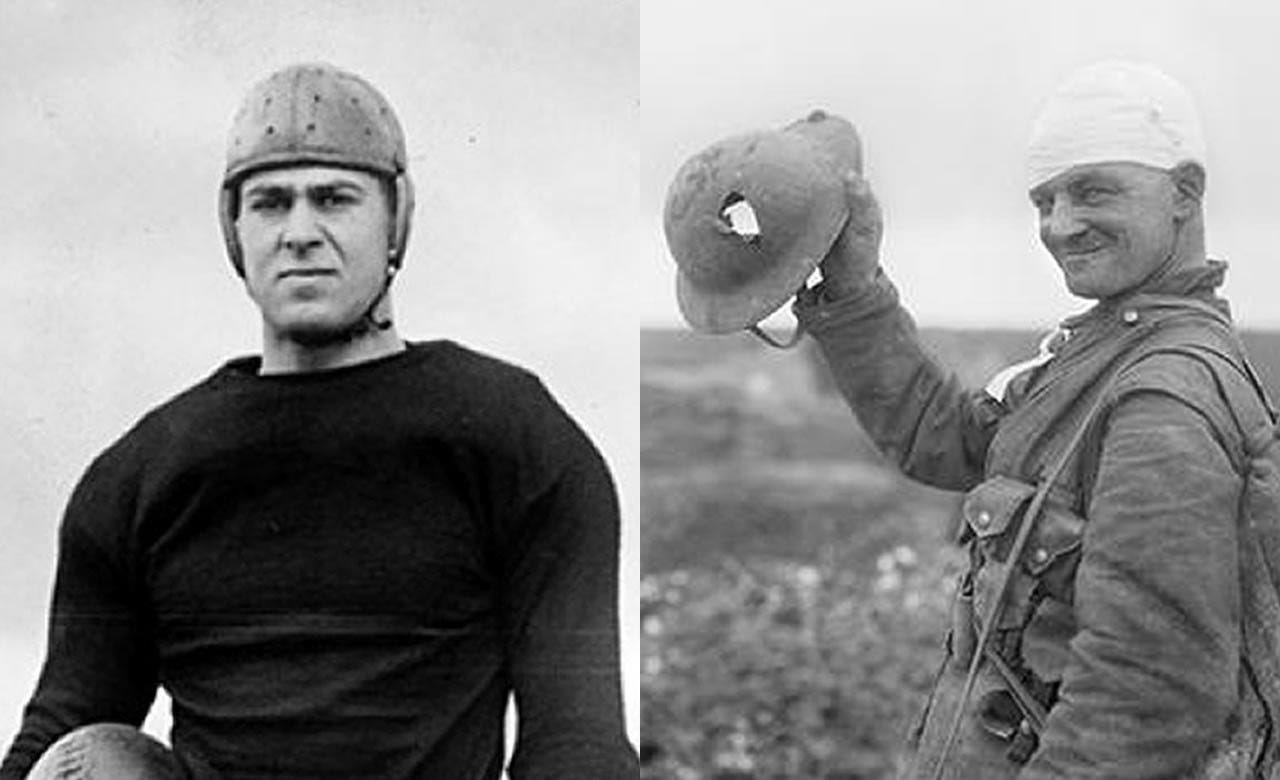
Standardized head protection appeared on the football field and the Western Front at the same moment in 1915.
Our brains have never recovered.
“How many fingers am I holding up?” the team doctor asked, h…
